The branch of therapy that deals with anticipated loss due to death is a specialization that often gets overlooked. As a counselor who works with anticipatory grief and has five years’ experience in a hospice bereavement office, I have found that primary caregivers usually need guidance and support but don’t ask for it until they are completely overwhelmed. Counseling for end-of-life caregiving is very much an area in which good therapists can make the difference.
Current Medicare standards for hospice do not cover the cost of a bereavement specialist for family members of a dying patient. Unless the family or caregiver seeks an outside therapist, chaplains and social workers affiliated with assisted living facilities or hospices become the de facto mental health experts, juggling family dynamics, anticipatory grief, medical regulations, spiritual concerns and the patient’s care plan.
Caregivers: The unsung heroes
Whether end-of-life care is being given in a home or a facility, caregivers can grow overwhelmed by the physical and emotional toll of their responsibilities. They may start showing signs of anticipatory grief, including mourning the loss of their role and relationship and fearing the future. This can be coupled with anger at the isolation and abandonment by others, bitterness at the exhaustion, frustration at the never-ending demands, shame for wishing caregiving were over already (which would mean the patient’s demise), helplessness at being unsure about what they should be doing and sadness at the way that time is running out.
In my book Take My Hand: The Caregiver’s Journey, Chris Renaud-Cogswell offered written reflections on her emotional overload with caregiving responsibilities: “I’m so jealous of all of you who enjoy your parents’ company and treasure the time you have with them. When do I get past the ‘I can’t believe this is my life,’ regretful, resentful stage? I have never used the F-word as much as I do since my mother moved in.”
Guilt seems to be the emotion that rises to the surface most often for caregivers. Even in the most “functional” homes, the intensity of caregiving can be enormous. For example, a spouse may not be capable of doing everything but still feels responsible for the care of his or her sick partner. Conversely, partners in good health may feel weighed down by the extreme change in their role and lifestyle. Adult children who are working or raising kids themselves can feel put upon to do more and angry that their time is so limited. Those caring for an elder may find old childhood resentments bubbling up. Relatives who might like to visit don’t know how to help. Asking for help triggers additional feelings of guilt and frustration among caregivers.
most “functional” homes, the intensity of caregiving can be enormous. For example, a spouse may not be capable of doing everything but still feels responsible for the care of his or her sick partner. Conversely, partners in good health may feel weighed down by the extreme change in their role and lifestyle. Adult children who are working or raising kids themselves can feel put upon to do more and angry that their time is so limited. Those caring for an elder may find old childhood resentments bubbling up. Relatives who might like to visit don’t know how to help. Asking for help triggers additional feelings of guilt and frustration among caregivers.
As grief counselors, we listen to recitations based on a lifetime of behaviors and try to help put boundaries in place. We validate and remind clients that they are doing the best they can under trying circumstances. Caregivers may struggle with the history of a poor relationship with the patient. These interpersonal dynamics are likely to continue being problematic. For many families, a storybook resolution or a full sense of forgiveness might be difficult to achieve.
One middle-aged man paid a daily visit to his dying father, who had a long history of being abusive and battling alcoholism. Despite the visits lasting for four or five hours, the man refused to interact with his father. Instead, he sat in a chair, played games on his phone and felt guilty. A daughter who had been constantly rejected by her narcissistic mother reacted by directing her frustration at staff for any minor infractions, fearing that her mother, who was dying, would deride her for her own lack of attention. In another case, an adult daughter wanted to scream at her mom for never asking for what she needed, acting out passive-aggressive patterns and playing the “martyr.” The daughter hated the nagging person she was becoming.
Caregiving can be a long journey, so, as counselors, we must explain the necessity of self-care for the caregiver. Even among caregivers who are fully engaged with their sick loved ones and content with their position, emotional exhaustion takes a toll. Whether dealing with a loved one’s personality changes or the loss of that person’s physical abilities or mental acuity, being on call as the “responsible adult” is draining. Caregiving can run the gamut of emotions and experiences, from boring to terrifying.
Self-care for caregivers includes asking for help, making schedules, sleeping, taking time alone, exercising, seeing friends, checking out support groups, praying, laughing, journaling, connecting through social media and, of course, learning to accept help. By presenting family members, friends, faith organizations or neighbors with specific ways to help, the caregiver is actually providing a service. Rather than viewing these “asks” as a burden to others, it can be reframed as an opportunity for others to do a good deed for the person who is dying.
A caregiver’s functions will depend on many variables. For instance, if the person who is dying is in a facility, the caregiver may be tasked with doing laundry, attending functions at the facility, visiting the sick loved one daily or weekly, finding coverage for meetings with facility staff to discuss behavior changes or concerns, driving the loved one to outside medical appointments, scheduling visits from friends and relatives, and maintaining a family home.
For at-home caregivers, responsibilities might include adjusting for safety precautions around the home. This might involve installing grab bars, removing throw rugs and acquiring nonslip mats, having a working fire extinguisher, checking that the water heater thermostat is set below 120 degrees Fahrenheit and preparing for durable medical equipment (such as commodes, hospital beds and oxygen tanks/cylinders). In addition, these caregivers typically shoulder the responsibility for being available to drive the person to appointments as necessary, finding coverage when away from the home and providing meals that are dietarily different.
Counselors should remind clients who have caregiver responsibilities that friends or relatives might be able to visit or engage in crafts or music with a sick loved one, thus allowing the caregiver some time off. To ward off burnout, caregivers need respite.
Thus we arrive at the conundrum of respite: “If I go away for a few days, what if my loved one dies? How will I live with the guilt?”
There are two scenarios at the end of life: One, the loved one dies when someone is with them and, two, he or she dies when no one is there. Caregivers often worry that their loved one might be alone when they die. Some hospices can provide 11th-hour care, during which volunteers can sit at bedside if the family wishes.
My experience in hospice has been that some patients follow a definitive trajectory in their decline, whereas others follow an indeterminate timeline, making a family’s desire to be bedside at the last breath fraught with uncertainty. Although many cultures encourage “vigiling” at the deathbed, there is an unknown: Does the patient want the family there? Some individuals need to be alone when they die and will release from this life only when the family or a specific person leaves. The speculation about why this happens is endless, but it may help alleviate family guilt to use the metaphor of a group coming to a bridge together, but because only the dying individual may cross that bridge, he or she will do it alone.
Family dynamics
As counselors, we should encourage caregivers to see that a document such as Five Wishes (fivewishes.org) is completed while the elder is mentally competent. This document serves as a directive about how the patient wishes to be cared for at the end of life. It is a binding document like a living will. In considering end-of-life protocols, all adults should be encouraged to write down their wishes so that these are known in advance.
During a crisis or major upset in a family system, different personality traits come to the fore. Family members who aren’t the primary caregiver might assume many roles at the end of life: the Swooper, the Know-It-All, the Call-Me-If-You-Need-Me sibling, the I-Don’t-Know-Anything-About-Dying-Elders family member … All the family roles are intensified. Folks who have a personal need to make amends come crashing in. The Golden Child comes back for a weekend and questions everything that’s been done.
Renaud-Cogswell shared her experience in Take My Hand: “Mom was diagnosed with lymphoma a week and a half ago. The hospice team began coming to care for her at our house shortly thereafter. Brother wants to take mom to lunch. Incredulous, I tell him she is sick, she has lymphoma, and that he could bring lunch here. He brings lunch. He doesn’t, however, bring lunch for me. Not something I should be overly surprised by, but I am hurt nonetheless. Then brother asks Mom if she would like to move into his empty townhouse. (Alone.) Then he and his girlfriend begin telling her all the positives about moving in there. I say, ‘She’s sick. She needs 24-hour care.’ Brother says, ‘Since I kicked my renters out, I need the money.’
“Loudly enough for them to hear, but soft enough so that Mom doesn’t, I hiss, ‘She’s dying!’ Then what do you suppose this brother asks our mother? ‘Can I borrow $500?’ (Who asks their dying mother for money???) And do you know what? She gives it to him! This was yesterday. I ran from the minute my feet hit the floor in the morning till my head hit the pillow at midnight last night. I need to sit down and have a good cry, but today, I’m afraid, will be just as busy.”
There are additional complications that must be addressed when “helpers” come. For caregivers, it is a frustrating and delicate struggle between wanting support and allowing helpers to make mistakes while visiting. The strain of feeling that no one else can do the caregiving correctly is immense. Caregivers should establish safety rules that are nonnegotiable — for example, the parent cannot go out without oxygen, medications must be administered on time, hospice will be called if the elder falls.
Grief counselor David Maes created a template (see below) that can be used when conflict arises between family members. The template helps ensure that during a family meeting, the identified patient remains the center of attention. Family members respond to prompts written in the appropriate boxes. Other concerns are written outside the square in list format.
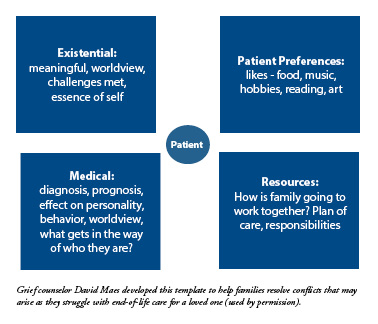
Start by asking the existential questions (the upper left-hand box): What is meaningful for the patient? Before the illness, what was the person’s worldview? How did he or she move through life? What was the essence of who they were? Next, move to the upper right-hand box, which deals with patient preferences. Ask what the person likes related to music, food, art, reading, nature, hobbies, etc.
The lower left-hand box deals with the illness: How is the diagnosis and prognosis affecting the loved one’s personality, behavior, likes and worldview? What gets in the way of who they are? Finally, list the resources: How is the family going to work together? What’s the plan of care? Who is responsible for what?
Counselors might need to remind family members that past relationship dynamics should have little bearing on the here-and-now focus of the discussion. The question to ask is, “Whose death is this anyway?”
Another protocol, from Susan Silk and Barry Goldman, is called Ring Theory (see tinyurl.com/RingTheory). In this exercise, the center circle is the patient, the subsequent circle is the primary caregiver and concentric circles can identify others who are less involved with daily care. The idea is that only comfort can go inward while the difficult emotions go outward. Family members and friends can offer unconditional love to each inner circle while finding their own support and a place to vent in extending circles. Each family member may find their own rings of support.
If end-of-life care is an area you are considering as a professional counselor, begin by learning about grief and bereavement. Alan Wolfelt’s comprehensive books are available through the Center for Loss & Life Transition (centerforloss.com). The Hospice Foundation of America also offers excellent webinars and books (hospicefoundation.org). There may be local support groups for caregivers in your area, and we should also be able to direct clients to resources such as the Alzheimer’s Association (alz.org) and AARP (aarp.org).
Competency in serving caregivers and families at the end of life involves a combination of approaches. We should be able to provide psychoeducation on dying and the needs of the dying. We should be competent listeners, validating and normalizing their experiences while encouraging life review and memory making. We can offer facilitation for family discussions. We can help our clients with boundaries, rituals and support groups. Finally, we can encourage the caregiver to engage in self-care, including therapy.
****
Tia Amdurer is a licensed professional counselor and national certified counselor with a private practice, Heartfelt Healing Counseling, in Lakewood, Colorado, that specializes in grief, loss, life transitions and trauma. She is the author of Take My Hand: The Caregiver’s Journey, which was published last year (TakeMyHandJourney.com). Contact her at tiaamdurer@gmail.com.
Letters to the editor: ct@counseling.org
Counseling Today reviews unsolicited articles written by American Counseling Association members. To access writing guidelines and tips for having an article accepted for publication, go to ct.counseling.org/feedback.
****
Opinions expressed and statements made in articles appearing on CT Online should not be assumed to represent the opinions of the editors or policies of the American Counseling Association.
Comments are closed.