Therapy must always be tailored to the individual; there is no one-size-fits-all model. However, certain approaches have been empirically verified for use with a variety of clientele. It is critical that all counselors, especially those working with client populations that are oppressed, have both an overview of evidence-based practices and specific techniques related to these approaches in their clinical toolboxes to help them provide the best counseling services possible.
Counselors are frequently required to use evidence-based practices and need to know how to use them effectively in counseling clients who are oppressed. Specifically, the unique development of the therapeutic relationship between oppressed clients and privileged clinicians must be understood and addressed. Multicultural counseling experts Derald Wing Sue and David Sue maintain that the dynamics of oppression shift the influence of the therapeutic relationship. Thus, counselors must alter their application of evidence-based practice techniques.
Solution-focused brief therapy and low socioeconomic status
Take a moment to think about what the basic needs of your own life are. What is impossible for you to live without? For many of us, our basic needs are continually met. Therefore, they often go unnoticed — they are woven into our everyday lives and ways of being in the world.
For others, questions such as “Will I eat today?” or “Will I have a safe and warm place to sleep tonight?” are asked daily. Often, the answer is “no.” Concerns such as clean drinking water, access to hygiene products and finding adequate shelter affect an inordinate number of individuals in the United States. School counselors and licensed professional counselors have a moral and ethical obligation to address these matters, with the intention of removing barriers and cultivating a safe space for clients in both the therapeutic relationship and the environment beyond our office walls.
Glenda Johnson (one of the co-authors of this article) worked as a school counselor and an advocate in a school system in which the majority of students came from low socioeconomic status (SES) backgrounds. Many of the students were on free or reduced lunch plans because their families’ financial resources were severely limited. At the core of Johnson’s work was the intent to ensure that every child’s basic needs were met while they were at school. She emphasized the importance of working collaboratively with other school staff members to build a team and a foundation for connecting these students and their families to resources.
It is also vital to assess an individual’s behaviors, emotions and reactions through a holistic, biopsychosocial approach rather than focusing only on the school context. Learned behavior concerns, inattention, difficulty with emotion regulation (anger), sadness and loss of hope are often the result of a lack of resources. Johnson recalls that if a student acted out, one of her first questions would be, “Did you have breakfast this morning?”
Johnson shares an anecdote that highlights the powerful act of providing a safe, therapeutic space for students to identify and voice their emotions openly with peers. As a school counselor, she infused the identification of various emotions into a game of musical chairs, and what transpired was completely unexpected. A student identified a “sad” emotion and explained that their father recently had lost his job. The student was experiencing fear about not having enough food to eat during this time. Then, other students began to share similar stories without prompting. The game of musical chairs transformed into a collaborative and touching experience as the students identified common ground and connected on deeper levels of understanding and empathy.
When providing services to individuals from a low SES, counselors may find it helpful to use a strengths-based therapeutic approach. The evidence-based practice of solution-focused brief therapy (SFBT) zeros in on the therapeutic relationship and the clinician’s way of being. In this relationship, there is an acknowledgment of reality but also an emphasis on solution-focused thought and reframing. Focusing on strengths, the counselor and client work together to identify and move toward making small changes in any area because a small change in one area often leads to change in another area.
SFBT often introduces the “miracle” question: “Suppose that when you go to sleep tonight, a miracle occurs that solves your problem, but because you were sleeping, you did not realize what happened. When you wake up in the morning, how will you realize a miracle happened? What will you notice that you are doing differently?” These questions enhance and expose glimpses of solutions that an individual may struggle to identify in everyday life situations.
 Additionally, SFBT places great value on successes. The counselor and client celebrate achievement and may use scaling to note the client’s progress. When working in a school system, the counselor could develop a creative and motivating way for children to rate themselves and their progress toward goals. For example, Johnson created a rating scale, complemented by the colors green, yellow and red, for kindergartners and first-graders. Green identified a completed goal, yellow identified progress toward a goal and red identified room for improvement. Similarly, she used a rating scale of 1-5 for students in second through fourth grades. Under this scenario, a student could check in with a rating, such as, “I am at a 3 and working toward a 5.” The counselor might respond, “What would it take to get to a 3.5?” The scale provided a visual for children to identify, track and celebrate their successes.
Additionally, SFBT places great value on successes. The counselor and client celebrate achievement and may use scaling to note the client’s progress. When working in a school system, the counselor could develop a creative and motivating way for children to rate themselves and their progress toward goals. For example, Johnson created a rating scale, complemented by the colors green, yellow and red, for kindergartners and first-graders. Green identified a completed goal, yellow identified progress toward a goal and red identified room for improvement. Similarly, she used a rating scale of 1-5 for students in second through fourth grades. Under this scenario, a student could check in with a rating, such as, “I am at a 3 and working toward a 5.” The counselor might respond, “What would it take to get to a 3.5?” The scale provided a visual for children to identify, track and celebrate their successes.
In SFBT, the counselor acknowledges client strengths and walks alongside these clients as they create and work toward their goals and future successes. “Flagging the minefield” is another technique counselors can introduce to help clients generalize and apply what they learn in counseling to future situations. Flagging the minefield is a particularly important facet of SFBT because it assists individuals in recognizing potential obstacles or barriers that will appear in their lives. The counselor and client work together to identify tools and resources the client can apply in other settings and relationships.
When working with students living in poverty, counselors should introduce a strengths-based approach and identify and gather resources to assist students and their families in removing barriers and meeting basic needs. Cultivating a safe, therapeutic relationship with students that focuses on solution building can assist them in building a stronger sense of self.
Motivational interviewing, SFBT and rural adolescent substance abusers
Adolescence is a vulnerable time and a critical period for developmental outcomes. During this stage of life, adolescents are exploring and forming their peer relationships and personal identities while beginning to distance themselves from family. Experimentation with substances often begins during this time. In 2012, Tara Carney and Bronwyn Myers found a correlation between the early onset of substance use and an elevated risk for later development of substance use disorders. Additionally, because early substance use may impact the growth of the adolescent brain, it has the potential to heighten one’s risk for delayed social and academic development.
Adolescents living in rural areas are marginalized in multiple ways. Children are an underserved minority population, as are rural populations. Sheryl Kataoka, Lilly Zhang and Kenneth Wells (2002) found that among youth with a recognized mental health need (estimated at 10 million to 15 million people), only 20-30 percent receive specialized mental health care. Rural communities are more likely to have fewer clinicians or require a long drive to see those clinicians, making it more difficult to obtain care. These disadvantages are exacerbated by the tumultuous nature of adolescence.
Motivational interviewing and brief interventions are two evidence-based practices particularly suited to this population because these approaches are generally influential in their therapeutic role while also being cost-effective. Motivational interviewing facilitates behavior change through exploration and resolution of ambivalence, and it focuses on being optimistic, hopeful and strengths-based. It uses principles of empathy, discrepancy, self-efficacy and resistance, and offers specific techniques such as OARS (Open questions, Affirmations, Reflective listening, Summarizing). SFBT emphasizes solutions, changes clients’ perceptions and behaviors, helps clients access their strengths and uses techniques such as exception to the problem, specification of goals and the miracle question.
Individual interventions with the use of the same interventions for multiple sessions are ideal, and research suggests that the earlier the intervention, the better the outcome. Early intervention shows better results than both preventive measures and later interventions because it reduces the need for more specialized interventions and provides applicable and useful tools and tactics for adolescents as they enter into various student, peer, familial and professional roles.
Challenges certainly exist when working with children and adolescents, particularly because many biological, environmental and social shifts occur organically during this time. As children and adolescents rapidly transition on a continuum of development, they become “moving targets.” Interventions that prove effective for those ages 11-12 often cease to be effective by ages 13 or 14. It is vital that counselors remain aware of this across the life span. Although adolescents are beginning to distance themselves from their caregivers, familial relationships and parental involvement remain crucial during this period.
To appropriately and competently involve the families of rural adolescents, some understanding of cultural values is necessary. In 2005, Susan Keefe and Susie Greene identified core Appalachian values, including egalitarianism, personalism, familism, a religious worldview, a strong sense of place and the avoidance of conflict. In the Appalachian region, assuming authority without demonstrating an authoritarian attitude is important. Language tends to be simple, direct, honest and straightforward. Family is extremely important, exemplified by the adage “blood is thicker than water.” Individuals’ relationship to the land is complex, and it can be beneficial to explore how clients view economic deprivation. In 2016, Sue and Sue also pinpointed some tendencies of rural clients, including having a “street-smart” attitude and way of being, depending on systems due to living in poverty and valuing survival at all costs.
As a result, subtle techniques such as stages of change, motivational interviewing and SFBT may be useful for this population. In stages of change, the intervention is matched to the stage of the client’s readiness to change (precontemplation, contemplation, preparation, action, maintenance, termination). Motivational interviewing facilitates an invitation to engage, and its strengths-based, hopeful tone can be helpful for clients living in an environment populated by deficits such as poverty and lack of education. The practical nature of brief therapy fits well with the no-nonsense worldview of clients coming from rural backgrounds.
Unfortunately, published rural studies often focus on specific regions or populations. Few interventions have been tested in rural settings, and the evidence from systematic reviews is often too general and not specific to the rural context. Ideally, rural communities could review interventions tested with various target populations in a range of settings. Such information is not usually available, however, and the strength of evidence is unlikely to be the only factor considered in choosing an intervention. The research on rural adolescent populations is limited, and little consistency exists across studies related to measurement tools. Furthermore, disseminating evidence-based practices to schools, families and community settings in rural areas is difficult due to the lack of resources.
However, it is important to note that there have been great improvements in substance abuse treatment and prevention with children and adolescents who live in rural areas. A 2016 Monitoring the Future survey of eighth-, 10th- and 12th-graders by the National Institute on Drug Abuse found the lowest ever reported rates of use for all illicit drugs, including alcohol, marijuana and nicotine. As further research is conducted, it will be important to delve into this information to identify what is already working with these individuals and what can be improved to better serve them moving forward.
Evidence-based practices with transgender clients
Transgender individuals face discrimination on multiple fronts. Many experience familial rejection, unequal treatment, harassment and physical violence during daily living. The rate of substance abuse within the transgender community is three times higher than that of the general population. There is a profound lack of competent health care for transgender individuals, and the care that is available may be inaccessible to a majority of the transgender population. The rate of unemployment within the transgender community is also three times greater than that of the general population, due in part to factors such as workplace discrimination, poverty and homelessness. Transgender people also face discrimination and mistreatment in shelters.
With high rates of homelessness, substance abuse and mistreatment, transgender people also have frequent interactions with law enforcement, where they can be subject to police brutality and discrimination. Within the criminal justice system, a high rate of physical and sexual assault is perpetrated against transgender individuals, and they are often denied medical treatment while incarcerated or detained.
Poor health outcomes for transgender people correlate with risk factors such as economic and housing instability, lower educational attainment, lack of family support and other intersectional factors such as race, ethnicity, immigration status and ability.
According to the 2015 U.S. Transgender Survey, 18 percent of transgender people who sought mental health services experienced a mental health professional attempt to stop them from being transgender. This correlated with higher rates of serious psychological distress and suicide attempts and an increased likelihood of running away from home, homelessness and engaging in sex work.
Research conducted in 2015 by Samantha Pflum et al. emphasized the lack of access to transgender-affirming resources and communities for individuals living in rural locations. The history of mistreatment and abuse of lesbian, gay, bisexual, transgender and gender-nonconforming clients by medical and mental health professionals must be acknowledged. Gender and sexual minority clients still face discrimination within the helping professions, and for individuals holding multiple marginalized identities, these experiences are compounded.
Even well-meaning providers are likely to make mistakes when working with marginalized clients. According to Lauren Mizock and Christine Lundquist, one of these mistakes is education burdening, or relying on the client to educate the provider about transgender culture or the general transgender experience. Resources exist to facilitate competence in these areas, and clinicians have a responsibility to refrain from placing the burden of their education on the client.
Some counselors participate in gender inflation, or focusing on the client’s gender to the exclusion of other important factors. Other counselors engage in gender narrowing, applying restrictive, preconceived ideas about gender to the client, or gender avoidance, which involves ignoring issues of gender altogether. Gender generalizing occurs when a clinician assumes that all transgender clients are similar. Gender repairing operates from a belief that a transgender identity is a problem to be “fixed.” Gender pathologizing involves viewing transgender identity as a mental illness or as the cause of the client’s issues. Finally, gatekeeping occurs when a provider controls client access to gender-affirming resources.
Acceptance of a client’s gender identity is ultimately not enough to provide competent, affirmative services. Understanding the nuances of these common mistakes will help clinicians provide a safe therapeutic environment that is affirming of these clients’ identity and humanity.
The Association for Lesbian, Gay, Bisexual and Transgender Issues in Counseling (ALGBTIC), a division of the American Counseling Association, has developed competencies for counseling transgender clients (see counseling.org/knowledge-center/competencies) that focus on the following eight domains:
- Human growth and development
- Social and cultural foundations
- Helping relationships
- Group work
- Professional orientation
- Career and lifestyle development competencies
- Appraisal
- Research
Counselors can work within this framework to:
- Promote resilience by using theoretical approaches grounded in resilience and wellness
- Conceptualize the development of a transgender individual across the life span
- Understand internal and external factors influencing identity development
- Consider how identity interacts with systems of power and oppression (especially for minority transgender individuals)
- Examine counselors’ own internalized beliefs and how those beliefs affect attitudes toward transgender clients
- Reevaluate approaches to working with transgender clients as new research emerges
One intervention that has been identified for use with this population by Ashley Austin and Shelley Craig is transgender-affirmative cognitive behavior therapy (CBT). Transgender-affirmative CBT modifies CBT interventions to address specific minority stressors, such as victimization, harassment, violence, discrimination and microaggressions, that transgender people commonly face. This approach uses psychoeducation to help clients understand the connections between transphobic experiences and mental health issues such as stress, anxiety, depression, hopelessness and suicidality. Experiences are processed through a minority stress lens to help clients move from a pathologizing-of-self mindset to an affirming view of themselves as people coping with complex circumstances.
Clinicians are advised to affirm the existence of discrimination and to help these clients identify influences on their mental health by using the transgender discrimination inverted pyramid (see below).
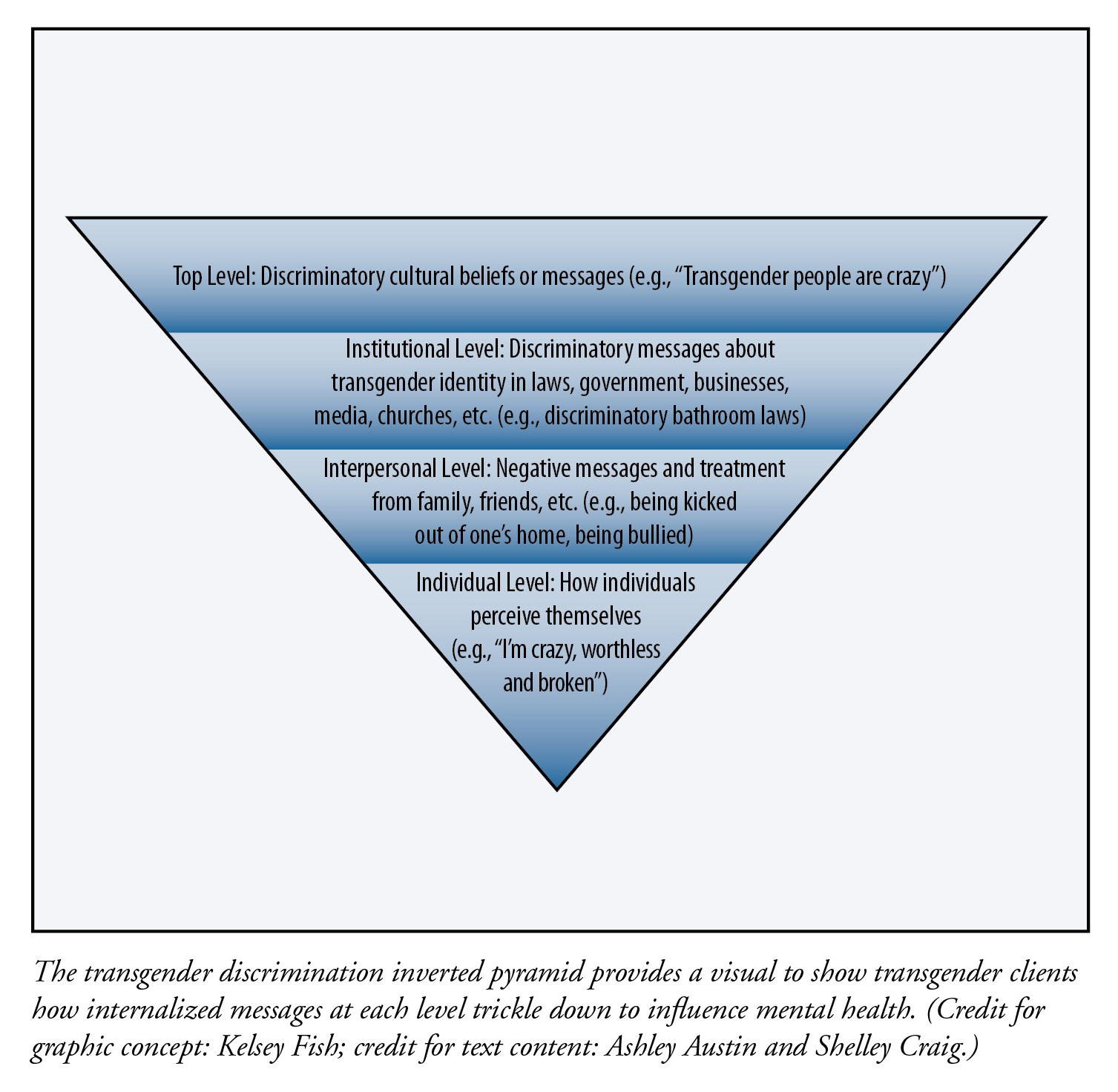
Transgender individuals internalize messages at each level, and it can be beneficial to have a visual for how these messages trickle down and influence mental health. Clinicians can empower transgender clients by assisting them in challenging internal and societal transphobic barriers. A few examples are challenging negative self-beliefs, connecting with a supportive community and advocating for self and community.
Another approach recommended for use with transgender clients by Joseph Avera et al. in 2015 is the Indivisible Self model, an Adlerian wellness model refined by Jane Myers and Thomas Sweeney that emphasizes strengths. There are five wellness factors of self in this model:
- Creative Self: Cognitions, emotions, humor and work
- Coping Self: Stress management, self-worth, realistic beliefs and leisure
- Social Self: Friends, family and love)
- Essential Self: Spirituality, self-care, gender identity and cultural identity
- Physical Self: Physical and nutritional wellness
This model easily can be adapted to a transgender-specific lens, especially regarding the Essential Self, by exploring gender and cultural identity and how they influence client experiences and beliefs. Used in conjunction with the ALGBTIC transgender competencies, the Indivisible Self model offers helping professionals both a conceptual and practical framework for working effectively with transgender clients.
For all clients, and transgender clients in particular, intersectional factors magnify the experience of oppression. Sand Chang and Anneliese Singh recommend addressing the intersectionality of race/ethnicity and gender identity for both clients and clinicians. This involves:
- Challenging assumptions about the experiences of transgender and gender-nonconforming people of color
- Building rapport and acknowledging differences within the therapeutic dyad
- Assessing client strengths and resilience in navigating multiple oppressions
- Providing a variety of resources that are affirming to transgender and gender-nonconforming people of color
In addition, assisting clients in locating social support is advised. Social support increases healthy coping mechanisms and helps with self-acceptance, thereby reducing psychological stress related to discrimination. Social support can also help to normalize and validate emotions related to discrimination.
Conclusion
Evidence-based practices have consistently been shown to be helpful to clients, but counselors must remember that they operate within the context of a relationship. To use evidence-based practices effectively, we must hold on to our humanness. The implementation of a single technique will look very different depending on who is in the room and what they are bringing with them.
Often, the expectations for using evidence-based practices might create pressure for counselors to follow a strict formula for treatment. Process variables such as honoring the personal relationship between the counselor and the client, maintaining a “therapist’s heart” and respecting the unique aspects of the client may seem to be at odds with the procedure for using a specific intervention. A working knowledge of multicultural issues can provide some context for how to shift evidence-based practices to fit the client rather than pressuring the client to conform to a prescribed, generalized format.
Using interventions with a solid evidence base is good practice. Adjusting their implementation on the basis of the unique identity of the person sitting across from us is great practice.
****
Knowledge Share articles are developed from sessions presented at American Counseling Association conferences.
Geri Miller is a professor in the Department of Human Development and Psychological Counseling (clinical mental health counseling track) at Appalachian State University (ASU) in North Carolina. She is a licensed professional counselor, licensed psychologist, licensed clinical addictions specialist and substance abuse professional practice board certified clinical supervisor. She has been a volunteer counselor at a local health department since the early 1990s. Her clientele has primarily consisted of women with little opportunity for jobs or education and who experience barriers of poverty. Contact her at millerga@appstate.edu.
Glenda S. Johnson is an assistant professor in the Department of Human Development and Psychological Counseling (school counseling program) at ASU. She is a licensed professional counselor and a licensed school counselor in North Carolina. Her scholarly focus includes school counselors delivering comprehensive school counseling programs, students who are at risk of dropping out of high school and the mentoring of new counseling professionals.
Mx. Tuesday Feral received their master’s degree in clinical mental health counseling and a certificate in systematic multicultural counseling from ASU. They are the support programs director for Tranzmission, a nonprofit organization serving the Western North Carolina nonbinary and transgender community through education, advocacy and support services. Tuesday offers training and workshops in trans cultural competence and cultural humility on local, state and national levels.
William Luckett received his master’s degree in clinical mental health counseling from ASU with a certificate in addictions counseling. He has interests in somatic therapy approaches, mindfulness, religious and spiritual topics in counseling, and substance abuse counseling. He currently provides in-home counseling to rural families in Virginia.
Kelsey Fish is a student in ASU’s clinical mental health counseling program and a clinical intern with Daymark Recovery Services in rural Appalachia. Her clinical interests include expressive arts therapy, adolescents, and gender and sexual minority issues.
Madison Ericksen is a graduate of the clinical mental health counseling program at ASU. She has specialized training and interest in trauma-informed practices that use mindfulness, eco-based and expressive art therapies as complementary treatments alongside traditional therapy. She provides strengths-based and resiliency-focused outpatient counseling for children and families.
Letters to the editor: ct@counseling.org
****
Opinions expressed and statements made in articles appearing on CT Online should not be assumed to represent the opinions of the editors or policies of the American Counseling Association.